Practice recommendations
- Malignant melanomas in situ can usually be treated in consultation with a specialist (C). Larger lesions may require referral.
- Based on best available evidence, surgical excision is the first-line treatment for most nonmelanoma skin cancers, with cure rates as high as 98% with proper margins (C).
- Consider Mohs surgery for larger lesions, sclerosing lesions with morpheaform histology, or for cosmetically sensitive areas (A).
- With properly selected lesions, curettage/electrodesiccation and cryosurgery have cure rates comparable to that of surgical excision (B).
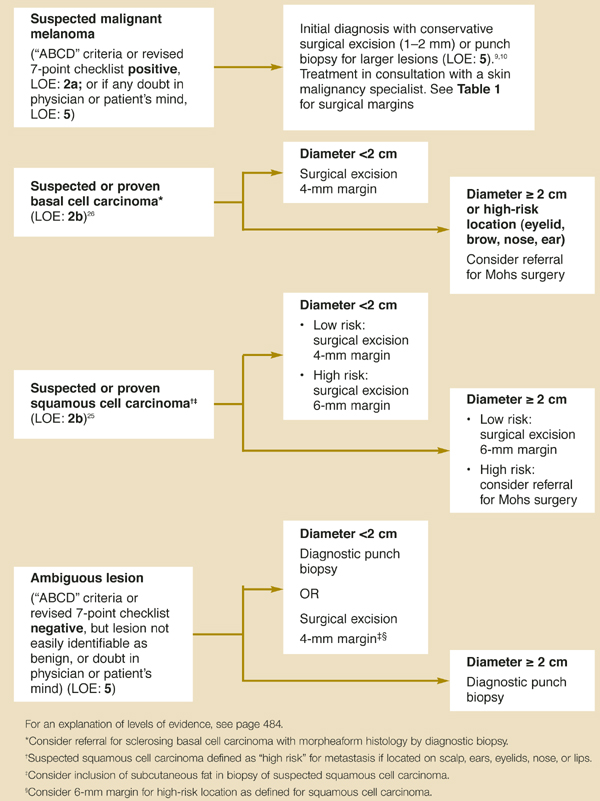
Reliable criteria exist to guide primary care physicians in the evaluation of malignant melanoma.1 Once a diagnosis of malignant melanoma is made, physicians should promptly consult with a skin malignancy specialist (Figure 1).
Several well-accepted treatment options exist for primary nonmelanoma skin cancer, but direct comparisons are lacking. The best evidence recommends surgical excision as first-line treatment for most nonmelanoma skin cancer. Cure rates up to 98% can be expected with appropriate margins.
Curettage/electrodesiccation and cryosurgery are probably equally effective with properly selected lesions. Physicians should be aware of those cases when nonmelanoma skin cancers are at higher risk for recurrence or metastasis and tailor their treatment plan accordingly.
Mohs micrographic surgery is the preferred treatment for high-risk and recurrent primary nonmelanoma skin cancer.
In this Applied Evidence review, we examine the guidance that can be gleaned from currently available evidence, and review each option in detail.
FIGURE 1
Surgical excision of suspected skin malignancies
Confirming the diagnosis
Our previous article in THE JOURNAL OF FAMILY PRACTICE, “Diagnosing skin malignancy: Assessment of predictive clinical criteria and risk factors,”1 presented a comprehensive review for the initial evaluation of skin malignancies. (This article is available online at www.jfponline.com.)
Nonmelanoma skin cancer includes basal cell carcinomas and squamous cell carcinomas. Nonmelanoma skin cancer, which accounts for most cases of skin cancer, has a high 5-year survival rate, more than 95%.2 Malignant melanoma represents only 1% of skin malignancies but leads to more than 75% of skin cancer deaths.3 Up to 83% of family physicians treat skin malignancies in their offices.4
When the diagnosis is uncertain on clinical grounds alone, an initial diagnostic biopsy may be used. Techniques include excisional, punch, and shave biopsies.
Excisional biopsy (Figure 2) is the preferred method for primary care evaluation of suspected skin malignancy (level of evidence [LOE]: 5).5,6 Excision wounds are easily cared for by patients and provide good cosmesis. Surgical excision may also be used for definitive treatment, as discussed below.
Punch biopsy or incisional biopsy (Figure 3) provides a full-thickness tissue sample with minimal scarring. A 3-mm punch is sufficient for most lesions (LOE: 5).5 Punch biopsy is a reasonable alternative when excision is impractical due to the size or location of a lesion.
Punch biopsy is not recommended if malignant melanoma is suspected by history or physical exam—an excisional biopsy should be done (LOE: 5).6 Even when performed mistakenly on a malignant melanoma, however, punch biopsy has not been shown to alter prognosis or cause dissemination of a tumor (LOE: 1b).7
Shave biopsies (Figure 4) are useful for benign-appearing lesions or elevated, nodular lesions suggestive of basal cell carcinoma or squamous cell carcinoma. Shave biopsy sites typically heal more slowly than excisional biopsies but do so with good cosmesis. In general, shave biopsy of pigmented lesions is contraindicated, but may be performed by an experienced physician confident of a benign clinical diagnosis. According to a National Institutes of Health consensus panel, suspected malignant melanoma should not be shaved, as the maximal depth of the tumor cannot be assessed.8
FIGURE 2
Excisional biopsy

FIGURE 3
Punch/Incisional biopsy
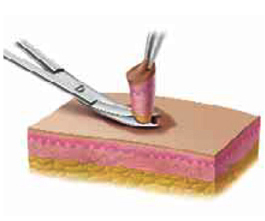
FIGURE 4
Shave biopsy

Malignant melanoma treatment
Overview
If a skin lesion is suspected clinically to be malignant melanoma, use the ABCD criteria and the revised 7-point checklist to guide biopsy decisions.1 If the physician or patient has any doubt, perform a biopsy.
If malignant melanoma is suspected, the initial biopsy should be conservative, with 1–2 mm margins (LOE: 5),9,10 and excisional, in order to determine the thickness of the tumor (Breslow’s measurement) and the histologic level of invasion (Clark’s level). Tumor depth at the time of diagnosis is the main factor guiding treatment and is the principal indicator predicting death due to malignant melanoma.8 Long-term survival of patients (10 years) with malignant melanoma <0.76 mm in thickness is greater than 90%; mortality rises linearly with increasing tumor thickness (LOE: 2b).11
Although knowledge of biopsy type is important for proper pathologic evaluation, it does not affect survival (LOE: 1b).7 Reviewing initial pathology results, a skin malignancy specialist (dermatologist, surgical oncologist, or plastic surgeon) can help determine the surgical margin necessary for curative excision. While most primary care physicians can treat lesions in situ, larger lesions require referral. Current recommendations for excision margins are shown in Table 1.