Two prospective studies found that anoscopy detects a higher percentage of lesions in the anorectal region than does flexible sigmoidoscopy (99% vs 78%).7,8 It is the procedure of choice for evaluating rectal diseases.
In skilled hands, anoscopy is safe; complications are unusual, and it can be performed in a physician’s office on short notice and without bowel preparation. After appropriate training, primary care physicians can perform routine examinations safely and accurately.
FIGURE 2
Anoscopy

The slotted anoscope provides the best visualization. Used with permission, National Procedures Institute, Midland, Mich.
Office-Based Treatment
Primary care physicians can safely use simple treatment measures to manage most cases of symptomatic hemorrhoids (Figure 3). Only the more symptomatic patients require surgical intervention.
Patients should be made aware of the nature of the condition and the advantages and disadvantages of the different treatment options. The evidence regarding these treatments is summarized in the Table.
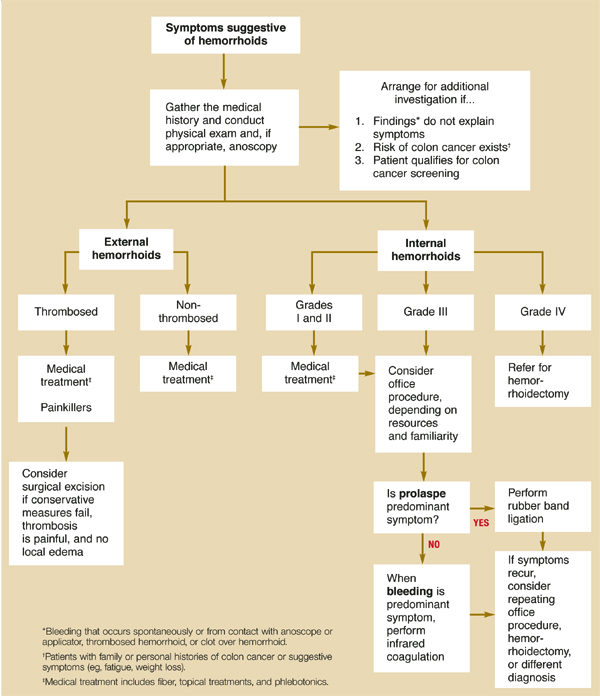
FIGURE 3
Management of adult patients with hemorrhoids
TABLE
Medical and surgical treatments for hemorrhoids
| Treatment | SOR* | Indication | Comments |
|---|---|---|---|
| Analgesics and anti-inflammatories2 | D | Grades I–IV and thrombosed external hemorrhoids | No trials comparing analgesics with anti-inflammatories |
| Topical treatments with corticosteroids or anesthetics3 | D | Grades I–III | No controlled trials with placebo are available, but patients report empiric benefit with their use; use only for brief periods |
| High-fiber diet or fiber supplements10-13 | B | Grades I–II | NNT=2.8 for reduction of rectal bleeding and 3.6 for pain relief23 |
| Office procedures23-25 | A | Grades I and II that do not respond to medical therapy, and grade III | Rubber band ligation was more effective and required fewer additional treatments for symptomatic recurrence than did infrared coagulation (NNT=9) and sclerotherapy (NNT=6.9); but rubber band ligation produced more complications than did infrared coagulation (pain: NNH=6) |
| Phlebotonics14-21 | B | Grades I–II | Moderate reduction of duration of bleeding during acute episodes of internal hemorrhoids; conflicting results for other outcomes (pain and prolapse) |
| Hemorrhoidectomy24 | A | Grades II–IV | Hemorrhoidectomy is more effective than office procedures, but it is more painful and presents more complications; office procedures are cheaper and require no time off from work |
| Stapling technique31-36 | A | Grades III–IV | Stapling technique is as effective as hemorrhoidectomy, is less painful, and requires less time off from work; more long-term data are needed37 |
| *For an explanation of strength of recommendation, see page 379. | |||
| SOR, strength of recommendation; NNT, number needed to treat; NNH, number needed to harm | |||
Benefits of lifestyle changes
The main purpose of lifestyle changes is to minimize prolonged straining during bowel movements, which is thought to contribute to the development of hemorrhoids. Such changes include increasing the amount of fiber in the diet, which is especially helpful for grade I and II internal hemorrhoids. Preventing constipation also helps alleviate more severe hemorrhoids and can help to prevent future episodes.10
Ruling out colorectal cancer
Rectal bleeding can mask the diagnosis of cancer. The probability of colorectal cancer increases in the elderly, those with a family or personal history of colorectal cancer, and those with any other symptoms of colorectal cancer (fatigue, weight loss, palpable tumor, anemia). Patients at risk need a more thorough evaluation, including endoscopy, to rule out malignancy.9
It is important to document that observed hemorrhoids account for the bleeding episode (bleeding at the contact site with the anoscope or an applicator, thrombosed hemorrhoids, or a clot over the hemorrhoid).
Several clinical trials have reported the benefits of a high-fiber diet or fiber supplements compared with placebo in relieving pain, bleeding, and prolapse (strength of recommendation [SOR]: B).10-13 We found no studies comparing the different types of bulk laxatives.
Although the role of certain foods in the pathogenesis of hemorrhoids or their acute exacerbation is accepted empirically, this has not been proved. Also, no firm evidence to date shows that increasing physical exercise, limiting time on the commode, or improving local hygiene are beneficial. However, these measures are usually recommended because they have other health benefits or are thought to do no harm (SOR: D).
Medical therapy
No rigorous evidence exists to support the use of topical therapies, physical or pharmacologic (sitz baths, anesthetics, phlebotonics, corticoids, or ice). Most studies have employed poor methods, lacked placebo control, and addressed heterogeneous preparations with multiple associated components. It is therefore not possible to formulate firm recommendations.
Soothing agents. Popular topical soothing agents are often combined with corticosteroids or anesthetics and are available over the counter as creams or enemas. Many patients report some empirical benefit with their use, especially corticosteroids and anesthetics (SOR: D).3 Advise patients against prolonged use due to possible local allergic effects and sensitization of skin (SOR: D).
Phlebotonics. Several phlebotonics have been evaluated in the literature; diosmin is the best-studied agent, but it is not commercially available in the United States at this time. In studies of patients with acute attacks of internal hemorrhoids (grades I to II), the main perceived effect was reduced bleeding duration;14,15 the results were conflicting for other outcomes (mainly pain and prolapse)14-18 (SOR: B).