Key Points
- Select medication based on the type and severity of a patient’s acne, as well as the patient’s skin type: creams, lotions, or ointments for dry skin; solutions or gels for oily skin.
- Choose topical therapy whenever possible to minimize side effects.
- Allow 6 to 8 weeks for most treatments to work before deciding to try another regimen or add other agents.
The surest route to success in treating acne vulgaris follows 3 steps. First, establish the type and severity of acne. Second, select medication appropriate for the patient’s condition and skin type. In general, patients with oily skin benefit from solutions or gels, while those with dry skin do better with creams, lotions, or ointments.1 Third, educate the patient about the disease, the different types of medications and their side effects, and expectations for improvement that are realistic. Realistic expectations should enhance compliance and lead to the successful resolution of a debilitating disease.
Types And Severity Of Acne
There are 3 types of acne: comedonal, papulopustular, and nodular (Table 1), all of which result from a multifactorial pathophysiologic process in the pilosebaceous unit: (1) sebum production, (2) follicular hyperkeratinization, (3) proliferation and colonization by Propionibacterium acnes, and (4) the release of inflammatory mediators.2 The resulting lesions include noninflammatory open (blackheads) and closed (whiteheads) comedones, as well as inflammatory papules, pustules, and nodules.
Acne severity is rated according to the Combined Acne Severity Classification that classifies acne into mild, moderate, and severe, based on the number and type of lesions (Table 2).3 Determining acne type and severity serves as a guide to treatment (Table 3).
Table 1
Types of acne
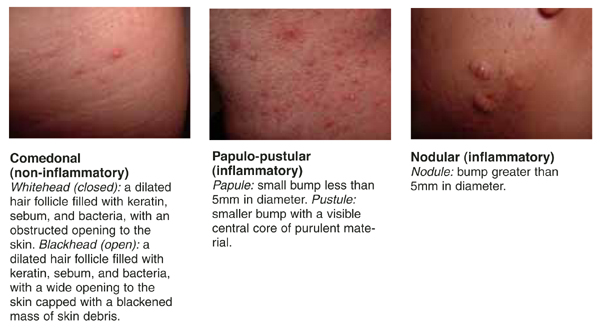
TABLE 2
Combined acne severity classification
| Severity | Definition |
|---|---|
| Mild acne | Fewer than 20 comedones, or Fewer than 15 inflammatory lesions, or Total lesion count fewer than 30 |
| Moderate acne | 20–100 comedones, or 15–50 inflammatory lesions, or total lesion count 30–125 |
| Severe acne | More than 5 nodules, or Total inflammatory count greater than 50, or Total lesion count greater than 125 |
TABLE 3
Treatment options based on type of acne
| Non-inflammatory acne | Inflammatory acne | ||
|---|---|---|---|
| Treatment | Comedonal | Papulo-pustular | Nodulocystic |
| Topical | |||
| Tretinoin (Renova et al) | X | X | |
| Benzoyl Peroxide | X | X | |
| Adapalene (Differin) | X | X | |
| Antibiotics | X | X | |
| Azelaic acid (Azelex) | X | X | |
| Tazarotene (Tazorac) | X | X | |
| Systemic | |||
| Oral contraceptives | X | X | X |
| Erythromycin | X | X | |
| Tetracycline | X | X | |
| Doxycycline | X | X | |
| Minocycline | X | X | |
| Isotretinoin (Accutane) | X | ||
| Adapted from Use of Systemic Agents in the Treatment of Acne Vulgaris, Am Fam Physician 2000;62. | |||
Treatment options
A variety of medications are available for the treatment of acne vulgaris. Note that most treatment regimens should be used for at least 6 to 8 weeks to judge their effectiveness before considering alternative treatments or adding other agents. The Figure 2, an algorithmic guide to the treatment of acne, represents the author’s assessment of the current literature. Alternative approaches may be appropriate after discussing options with individual patients. Table 4 summarizes the strength of evidence for acne interventions and how each compares with other treatments for the same type of acne.
Topical agents
Salicylic acid, found in a number over-the-counter cleansers, has both anti-inflammatory and mild comedolytic effects. It can be used as initial therapy for mild acne or as an adjunctive agent in a broader therapeutic regimen. In a placebo-controlled study of 114 patients, 2% salicylic acid lotion demonstrated a statistically significant improvement from baseline at 12 weeks (SOR: B).4 No side effect data were provided.
Tea tree oil comes from the Australian tree Melaleuca alternifolia and has had success anecdotally in treating various skin conditions. In a single-blind trial of 124 patients, 5% tea tree oil gel was compared with 5% benzoyl peroxide lotion in the treatment of mild-to-moderate acne. Both agents significantly reduced the number of inflammatory lesions and comedones (SOR: B).5 However, benzoyl peroxide was statistically superior to tea tree oil in reducing inflammatory lesions and had a faster onset of action. Encouragingly, patients treated with tea tree oil experienced fewer side effects.
Benzoyl peroxide (BPO) is a potent bactericidal agent with mild keratolytic properties. Several trials have shown the 5% concentration to be consistently superior to placebo at a statistically significant level in the treatment of mild-to-moderate acne, with a 30% decrease in lesion counts (SOR: A).6,7 In addition, two small trials involving 153 patients with mild-to-moderate acne compared the efficacy of different concentrations of topical benzoyl peroxide (2.5% vs 5% and 2.5% vs 10%) used twice daily.8 These trials demonstrated no differences in efficacy among the various preparations based on lesion counts, and there was no dose-response effect (SOR: A). Erythema and scaling occurred with almost identical frequency with the 2.5% and 5% concentrations but more often with the 10% concentration. Thus, the 2.5% and 5% concentrations appear to be preferable based on the balance of risks and benefits.
Topical tretinoin (Renova, Retin-A, Avita) is a comedolytic agent effective as monotherapy for noninflammatory acne. In two randomized controlled trials involving 292 patients of comparable age, use of 0.02% and 0.05% tretinoin strengths showed a statistically significant reduction in comedones and papules with a dose-response effect after at least 4 to 8 weeks of treatment when compared with placebo (SOR: A).9,10 However, there was also a statistically significant increase in erythema and peeling that was maximal after 1 to 3 weeks and decreasing thereafter. In addition, an exacerbation of inflammatory lesions (pustular flare) may occur within 2 to 4 weeks of onset of therapy.11