Deprecated function: Return type of DatabaseStatementBase::execute($args = [], $options = []) should either be compatible with PDOStatement::execute(?array $params = null): bool, or the #[\ReturnTypeWillChange] attribute should be used to temporarily suppress the notice in require_once() (line 2246 of /var/www/webmd/apps/mdedge/htdocs/includes/database/database.inc).
Deprecated function: Return type of DatabaseStatementEmpty::current() should either be compatible with Iterator::current(): mixed, or the #[\ReturnTypeWillChange] attribute should be used to temporarily suppress the notice in require_once() (line 2348 of /var/www/webmd/apps/mdedge/htdocs/includes/database/database.inc).
Deprecated function: Return type of DatabaseStatementEmpty::next() should either be compatible with Iterator::next(): void, or the #[\ReturnTypeWillChange] attribute should be used to temporarily suppress the notice in require_once() (line 2348 of /var/www/webmd/apps/mdedge/htdocs/includes/database/database.inc).
Deprecated function: Return type of DatabaseStatementEmpty::key() should either be compatible with Iterator::key(): mixed, or the #[\ReturnTypeWillChange] attribute should be used to temporarily suppress the notice in require_once() (line 2348 of /var/www/webmd/apps/mdedge/htdocs/includes/database/database.inc).
Deprecated function: Return type of DatabaseStatementEmpty::valid() should either be compatible with Iterator::valid(): bool, or the #[\ReturnTypeWillChange] attribute should be used to temporarily suppress the notice in require_once() (line 2348 of /var/www/webmd/apps/mdedge/htdocs/includes/database/database.inc).
Deprecated function: Return type of DatabaseStatementEmpty::rewind() should either be compatible with Iterator::rewind(): void, or the #[\ReturnTypeWillChange] attribute should be used to temporarily suppress the notice in require_once() (line 2348 of /var/www/webmd/apps/mdedge/htdocs/includes/database/database.inc).
Article
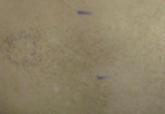
Linear Scarring Following Treatment With a 595-nm Pulsed Dye Laser
Both from the Division of Dermatology, David Geffen School of Medicine, University of California, Los Angeles. Dr. Ezra also is from the Department of Dermatology, Indiana University School of Medicine, Indianapolis. Dr. Behroozan also is from the Dermatology Institute of Southern California, Santa Monica, and the Department of Dermatology, VA West Los Angeles Medical Center.
The authors report no conflict of interest.
Correspondence: Daniel Behroozan, MD, Dermatology Institute of Southern California, 2221 Lincoln Blvd, Ste 100, Santa Monica, CA 90405 (db@dermsurgery.net).
Alternative laser treatment protocols have been proposed in the literature. Rohrer et al15 recommended multiple passes at subpurpuric doses for treatment of facial telangiectases with the PDL. It has been suggested that multiple stacked pulses at lower fluences may have similar effects on targets as a single pulse at a higher fluence, thereby minimizing thermal injury and leading to decreased risk for adverse events such as scarring. When treating vascular lesions such as telangiectases, increasing the fluence will increase the risk for purpura due to the constant pulse duration. Stacking pulses of lower fluence may have the advantage of heating vessels to a critical temperature without creating purpura, leading to similar clearance rates with decreased adverse risk profiles.15
It may be better to err on the side of safety by performing a greater number of treatment sessions with increased pulse width and decreased fluence (subpurpuric treatment settings) to minimize the risk for atrophic scarring from treatment with the PDL. Treating superficial facial telangiectases with a pulse-stacking technique may improve clinical results without a remarkable increase in adverse effects. It may be wrongfully intuitive to try to maximize results by using high fluences and purpuric narrow pulse durations; this case report reiterates the danger of using these settings in an attempt to rapidly achieve clearance of telangiectases. Lastly, this case underscores the value of verbal and written postoperative instructions that should be given to every patient prior to undergoing laser therapy. Specifically, with regard to our case, the laser operator must be aware at all times of potential adverse events, which may be foreseen during treatment if persistent or prolonged blanching and/or blistering occurs. The physician operator and patient must be prepared to rapidly respond to adverse reactions such as skin necrosis or blistering. Meticulous wound care is necessary if skin breakdown occurs. We recommend using a hydrating petrolatum ointment or a topical emulsion to minimize the risks for scarring, if possible.