According to the National Academy of Medicine (NAM), health literacy is “the degree to which individuals have the capacity to obtain, process and understand basic health information and services needed to make appropriate health decisions.”1 Studies suggest that millions of patients have inadequate health literacy and cannot make fully informed decisions because of this lack of knowledge.2-4 A 2007 National Patient Safety Foundation report calculated that inadequate health literacy burdens the U.S. health care system with an additional $106 to $238 billion annually.5
In 2014, the American Diabetes Association reported that diabetes affects 29.1 million Americans (9.3%) and that by 2050 1 in 3 Americans will have diabetes.6 People with diabetes have health care costs 2.3 times higher than the cost for nondiabetic patients. The cost of taking care of patients with diabetes annually is about $245 billion.6 Without interventions that address health literacy and effective self-management to reduce the risks of complications and comorbidity, health care costs related to diabetes will continue to increase.
Literature Review
According to a U.S. Department of Education assessment on adult health literacy in 2003, 88% of adults in the U.S. have inadequate health literacy.2 About 90 million Americans lack health literacy skills, according to a 2004 NAM report.3 Heinrich, who conducted a review of U.S. studies on health literacy, concluded that about 25% of Americans have low health literacy.4
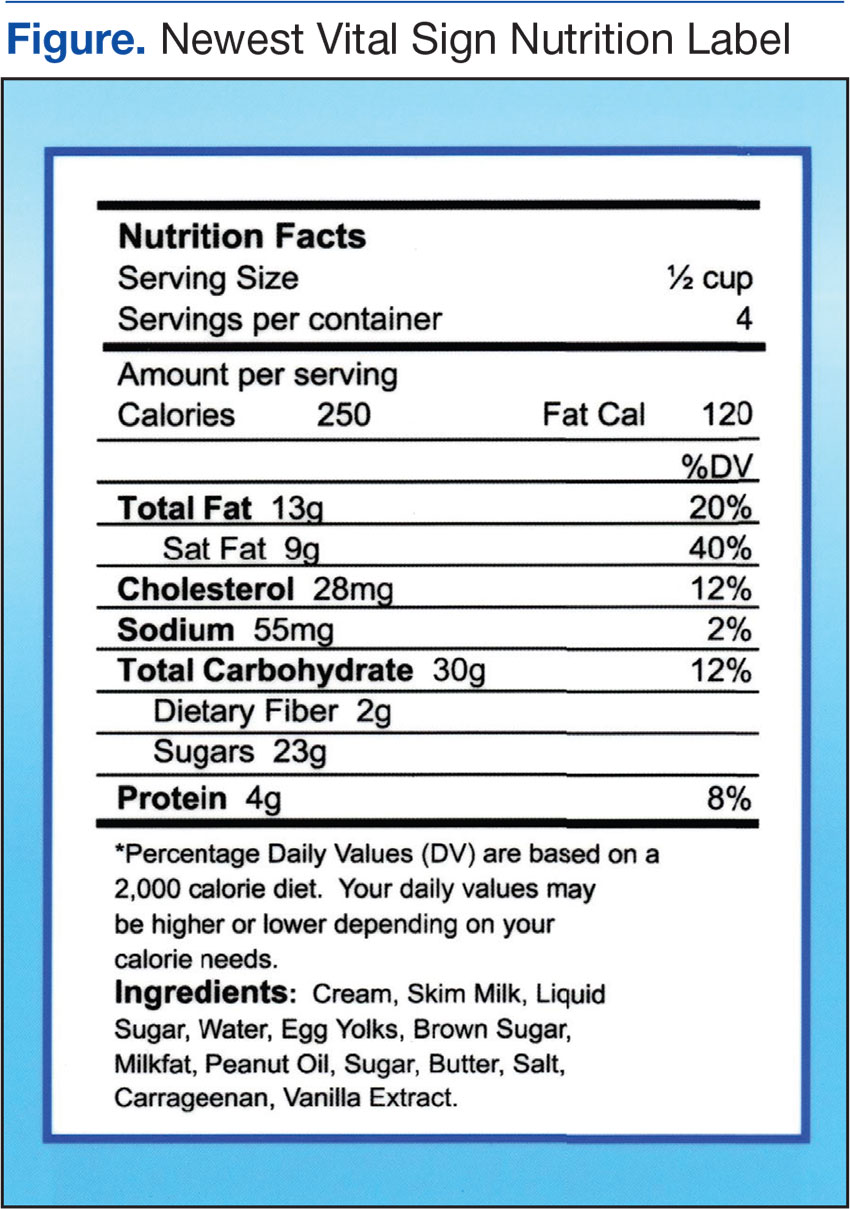
The Newest Vital Sign Tool
The Newest Vital Sign (NVS) tool is a free tool developed by Pfizer (New York, NY) for assessing health literacy. Participants are asked 6 questions about nutrition based on an ice cream nutrition label (Figure). The researcher records the participant’s responses, which accommodates participants who may have difficulty reading. The tool is scored from 0 to 6. A score of below 4 indicates the possibility of limited health literacy.7 This test can be completed in about 3 minutes, is widely accepted, and provides results comparable to more extensive literacy tests.8 A study conducted by Welch and colleagues suggested the NVS tool is both cost and time efficient.9 Ryan and colleagues found that 98% of patients in their study (n = 289) did not have objections to taking the NVS assessment.10
Escobedo and Weismuller’s study used the NVS health literacy tool to assess the health literacy of renal patients.3 In 2004, about 50,000 American patients with diabetes began treatment for kidney failure due to diabetes complications.6 Escobedo and Weismuller found that patients with diabetes with limited health literacy knowledge are more likely to be hospitalized, thus increasing health care costs.3 In addition, they discovered that these patients demonstrated poor adherence to prescribed treatment protocols. Welch, VanGeest, and Caskey conducted a case study on time, cost, and clinical utilization of the NVS health literacy tool and found that a patient’s lack of health literacy was linked to limited participation in personal medical decisions.7,9 Patient’s lack of knowledge was associated with delays in seeking treatment, poor self-management of the disease, and more hospital admissions.
Health Literacy and Diabetes
Studies specific to diabetes and inadequate health literacy support the premise that better health literacy leads to improved patient outcomes. Using the NVS tool, Heinrich conducted a study of the health literacy of 54 patients with diabetes in a primary care setting. The study showed that 65% had inadequate health literacy and that patients with diabetes with inadequate health literacy were more likely to have poor glycemic control compared with patients with diabetes and adequate health literacy levels.4 McCleary-Jones examined diet, foot care, and exercise of 50 African American participants with diabetes from a community health center, finding a positive relationship between health literacy and diabetes knowledge.11
Long and Gambling conducted a 2-year prospective, observational study that incorporated motivational interviewing and patient-centered care into a self-management program, examining the effectiveness of scheduled phone interventions to assist patients with diabetes in the management of their disease.12 The interventions used structured and consistent questions supported by a protocol and script that examined medication adherence and lifestyle choices. Long and Gambling concluded that “the findings demonstrate not only changes in the depth and detail of diabetes-related knowledge and confidence, but also enhanced competence in translating knowledge into every day self-care.”12 These researchers concluded that increased knowledge translated into better patient self-management of their disease. The Long and Gambling study included general self-management characteristics of monitoring HbA1c, diet, exercise, medication management, and general self-care. These researchers contend that diabetes self-management education must be a long-term endeavor to promote change.12
Mendoza and Rosenburg’s meta-analysis on self-management programs for diabetes and chronic conditions found a statistically significant 0.81% reduction in hemoglobin A1c (HbA1c). Characteristics of self-management programs that were linked to improved outcomes included nurse and provider education on medications, diet and/or exercise, and demonstrated use of motivational interviewing and biofeedback. Mendoza and Rosenburg suggested motivational interviewing focuses on the patient’s perspective and facilitates the process that the patient uses to assess their needs and to think about possible solutions.13 Mulimba and Bryo-Daniel found that motivational interviewing is a valuable tool for primary care nurses’ health promotion practice, and Thompson and colleagues found that it was effective in changing behavior.14,15
