Another population for whom cognitive screening may be appropriate is patients with certain medical conditions known to be associated with dementia, as well as any older person with unexplained functional decline. Examples of conditions associated with cognitive decline include Parkinson’s disease, a history of stroke, and diabetes mellitus.21-23
Most patients with memory difficulties and other cognitive problems do not report these complaints to their medical provider, and it is unrealistic to expect them to do so. Often it is a family member or a coworker who becomes aware of a problem and voices these concerns to the provider; however, the provider should not rely on this to ensure early detection.
Clinicians must be pro-active and maintain a high index of suspicion for cognitive difficulties, especially when treating adults older than 70 or 75. Becoming familiar with a variety of tools and using one or more regularly to determine whether an individual does or does not have cognitive changes that might warrant further assessment should be a routine part of care.
WHICH TEST TO USE?
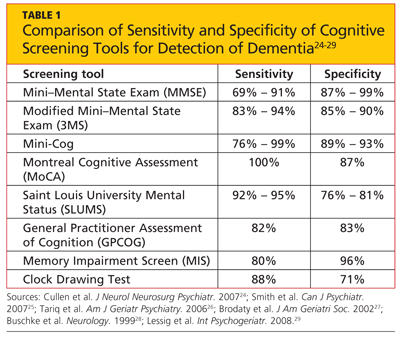
There is no single, ideal cognitive screening tool that can be recommended for use in every clinical setting. However, the ideal tool would have high sensitivity (ie, the proportion of those with impairment correctly classified as impaired), high specificity (the proportion of those who are unimpaired correctly identified as not having cognitive problems; see Table 1,24-29 below), and a high positive predictive value (proportion identified by screening as impaired who really have cognitive impairment). Additionally, such a tool should be easy to administer and score, and should take a minimum amount of time to conduct in our time-pressured clinical environment.
There is no single, ideal cognitive screening tool that can be recommended for use in every clinical setting. However, the ideal tool would have high sensitivity (ie, the proportion of those with impairment correctly classified as impaired), high specificity (the proportion of those who are unimpaired correctly identified as not having cognitive problems; see Table 1,24-29 below), and a high positive predictive value (proportion identified by screening as impaired who really have cognitive impairment). Additionally, such a tool should be easy to administer and score, and should take a minimum amount of time to conduct in our time-pressured clinical environment.
Many of the currently available cognitive screening tests overemphasize memory to the neglect of other areas of cognitive function, such as executive function, language, and praxis, which can be impacted in patients with various conditions.24 One review of cognitive screening tests suggests that a comprehensive screening instrument should include six core neuropsychologic domains that are most commonly affected in the early stages of different dementias:
• Executive function
• Abstract reasoning
• Attention/working memory
• New verbal learning and recall
• Expressive language
• Visuospatial construction.24
LIMITATIONS OF CURRENT SCREENING TESTS
Cognitive screening does involve some risk, and every tool has known limitations. A significant barrier can be the administration time required, possibly ranging from five to 20 minutes. There is a potential for false-positive results, and there can be distress and stigma associated with a diagnosis of dementia, for both patients and families.
Cognitive screening does involve some risk, and every tool has known limitations. A significant barrier can be the administration time required, possibly ranging from five to 20 minutes. There is a potential for false-positive results, and there can be distress and stigma associated with a diagnosis of dementia, for both patients and families.
The majority of cognitive screening tests were developed and validated using cohorts of English-speaking patients. When used in other populations, such as those with English as a second (or third) language, or when used in translation, the results may not be valid. Similarly, many tests have an inherent educational bias, presuming attainment of an eighth-grade level or higher—again calling results into question when the test is conducted in people with less formal education. Further, most of the currently available tools are insensitive to small changes, as they were designed for screening, not to detect changes in a patient over time.
Screening tests may have a ceiling effect, that is, they may be insensitive to changes among patients with high intelligence or high levels of education premorbidity. Some tests may also have a floor effect, lacking the ability to assess for change in patients below a certain level of education or intelligence. The summary scores of these tests have cut-offs for normal and may allow broad-range classification of levels of impairment as mild, moderate, or severe; this is not very useful in distinguishing different patterns of cognitive loss.
COGNITIVE SCREENING TOOLS
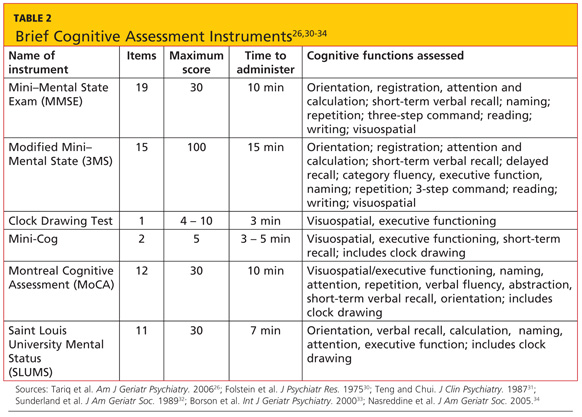
A variety of tools are available for bedside/clinical assessment of cognition (see Table 226,30-34 below). Their administration can be learned without difficulty, and they can be conducted with relative ease to provide insight into a patient’s cognitive abilities and deficits.
A variety of tools are available for bedside/clinical assessment of cognition (see Table 226,30-34 below). Their administration can be learned without difficulty, and they can be conducted with relative ease to provide insight into a patient’s cognitive abilities and deficits.
Mini–Mental State Exam
The most commonly used cognitive screening tool is the Folstein Mini–Mental State Exam (MMSE).30 With administration taking about 15 minutes, the MMSE includes assessment of attention, orientation, registration, recall/short-term memory, language, and visuospatial construction. Clinicians will find this tool most useful in assessing the individual with suspected early dementia and to follow progression through the early and middle stages of cognitive decline in those with Alzheimer’s disease and related dementing disorders.
The most commonly used cognitive screening tool is the Folstein Mini–Mental State Exam (MMSE).30 With administration taking about 15 minutes, the MMSE includes assessment of attention, orientation, registration, recall/short-term memory, language, and visuospatial construction. Clinicians will find this tool most useful in assessing the individual with suspected early dementia and to follow progression through the early and middle stages of cognitive decline in those with Alzheimer’s disease and related dementing disorders.