Authors’ Disclosure Statement: Dr. Kovar reports that he receives research support from a company or supplier as a principal investigator from DePuy Synthes, and other financial or material support from a company or supplier from OHK Medical Devices. Dr. Herzenberg reports that he is a consultant for Smith & Nephew, Ellipse Technologies, Orthofix, Orthopediatrics, and Wishbone Medical. He also reports that the following companies supported his institution's non-profit organization, which provides financial assistance to their patients: Stryker; Orthocare Solutions; Medevations; Bay Scribe; Nations Healthcare; and Chesapeake Surgical. The following companies supported Dr. Herzenberg’s institution's annual course for orthopedic surgeons: Smith & Nephew; BrainLab; Orthofix; DePuy Synthes; Stryker; Wright Medical Technology; Zimmer Biomet; and The MHE Coalition. Dr. Jauregui reports no actual or potential conflict of interest in relation to this article.
Dr. Kovar is an Orthopaedic Surgeon, Landesklinikum Baden-Mödling, Austria. Dr. Jauregui is an Orthopedic Surgery Resident, University of Maryland, Department of Orthopedics, Baltimore, Maryland. Dr. Herzenberg is Head of Pediatric Orthopedics, Sinai Hospital, and Director of the International Center for Limb Lengthening, Rubin Institute for Advanced Orthopedics, Sinai Hospital of Baltimore, Baltimore, Maryland.
Address correspondence to: John E. Herzenberg, MD, Rubin Institute for Advanced Orthopedics, Sinai Hospital of Baltimore, 2401 W. Belvedere Avenue, Baltimore, MD 21215 (tel, 410-601-9562; fax, 410-601-9575; email, jherzenberg@lifebridgehealth.org).
Am J Orthop. 2018;47(6). Copyright Frontline Medical Communications Inc. 2018. All rights reserved.
Florian M. Kovar, MD Julio J. Jauregui, MD John E. Herzenberg, MD . Accuracy of Distal Femoral Valgus Deformity Correction: Fixator-Assisted Nailing vs Fixator-Assisted Locked Plating. Am J Orthop.
June 12, 2018
References
In both FAN and FALP, the external fixator is applied and adjusted after the osteotomy for accurate alignment. In FALP, the plate is added without moving the leg from its straight position. However, in FAN, the knee must be flexed to 30° to 90° for insertion of the retrograde knee nail, and the alignment may be lost if the external fixation is not fully stable. Therefore, we hypothesized that FAN would be less accurate than FALP. Hence, the purposes of this study is to compare the correction achieved with FAN and FALP in patients with distal femoral valgus deformities and to describe the intraoperative complications associated with both techniques.
MATERIALS AND METHODS
After proper Institutional Review Board approval was obtained, a consecutive cohort of 35 patients who underwent femoral deformity correction with either FAN or FALP during an 8-year period (January 2002 to December 2010) was retrospectively reviewed. Eleven patients had to be excluded because of inadequate follow-up (<12 months) or because additional procedures were simultaneously performed. A total of 24 patients (27 femora) who had a mean age of 26 years (range, 14-68 years) were included in the final study cohort. Specifically, 20 femora (18 patients) were corrected using the FAN technique (7 males and 11 females; mean age, 36 years; range, 14-68 years), and 7 femora (6 patients) were fixed using the FALP technique (2 males and 4 females; mean age, 16 years; range, 15-19 years). The median follow-up in the FAN cohort was 5 years (range, 1-10 years), and the median follow-up in the FALP cohort was 5 years (range, 1-8 years) (Table 1).
Table 1. Study Details and Demographic Characteristics
The specific measurements performed in all patients were MAD, mechanical lateral distal femoral angle (mLDFA), and medial proximal tibia angle (MPTA). These were measured from standing anteroposterior radiographs of the knee that included the femur.21 All outcome data were collected from the medical charts, operative reports, and radiographic evaluations. To ensure accuracy, all measurements were performed by 2 authors blinded to each other’s measurements. If a variation of <5% was obtained, the results were averaged and used for further analysis. Whenever a difference of >5% was obtained, the measurement was repeated by both authors for confirmation.
SURGICAL FAN TECHNIQUE
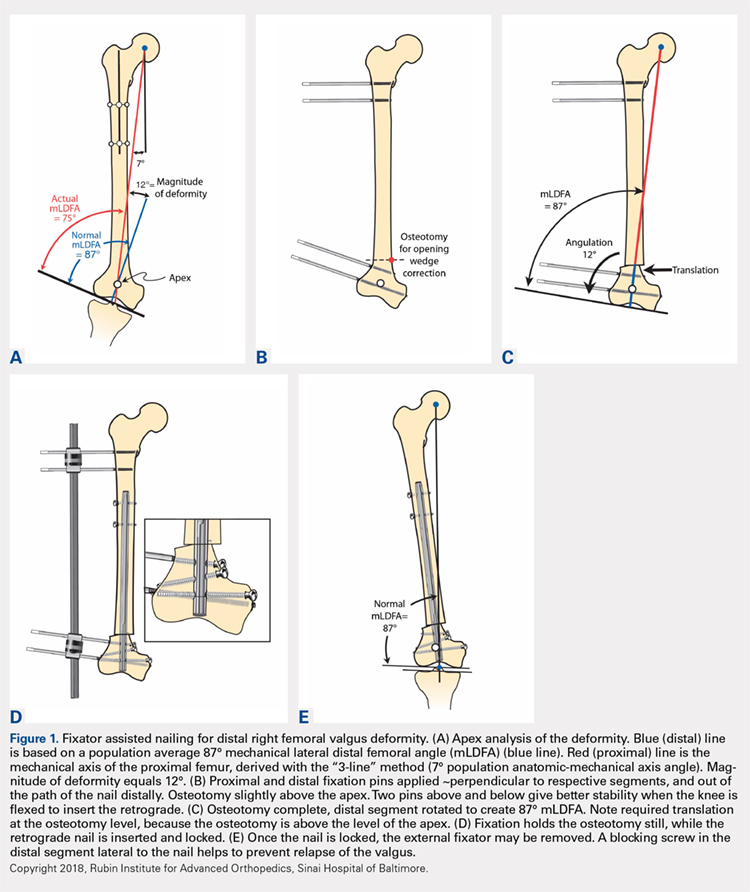
After measuring the deformity (Figure 1A) with the patient under general anesthesia on a radiolucent table, the involved lower limb is prepared and draped. Two half-pins are inserted medially, 1 proximal and 1 distal to the planned osteotomy site (Figure 1B), and then connected loosely with a monolateral external fixator. Special care is taken while placing the half-pins, not to interfere with the insertion path of the IM rod. When performing the preoperative planning, the level of osteotomy is chosen to enable the placement of at least 2 interlocking screws distal to the osteotomy. Then, a percutaneous osteotomy is performed from a lateral approach, and the bone ends are manipulated (translation and then angulation) to achieve the desired deformity correction. The external fixator is then stabilized and locked in the exact position (Figure 1C). Subsequently, retrograde reaming, nail insertion, and placement of proximal and distal locking screws are performed (Figure 1D). Blocking screws may give additional stability. The removal of the external fixator is the final step (Figure 1E).20