A Quality Improvement Initiative to Improve Emergency Department Care for Pediatric Patients with Sickle Cell Disease
Journal of Clinical Outcomes Management. 2014 February;21(2)
References
Secondary analyses were conducted to evaluate whether mean pain scores were significantly different over the course of the ED visit for the 78 unique patients seen post order set implementation. A multivariable mixed linear model, for the outcome of the third pain score, was used to assess the associations with prior scores and to control for potential covariates (age, gender, number of ED visits, hemoglobin type) that were determined in advance. A statistical significance level of 0.05 was used for all tests.
Results
Baseline data were collected from December 2011 to May 2012. The protocol was implemented in July 2012 and was utilized during 165 ED visits (91% of eligible visits) through April 2013. There were no statistically significant differences in demographic or clinical characteristics between the 55 patients whose charts were reviewed prior to implementing the order set and the 78 unique patients treated thereafter. Pre order set implementation, the mean age was 14.6 ± 6.4 years; 60% were female and the primary diagnosis was HgbSS disease (61.8% of diagnoses). Post order set implementation, the mean age was 16.0 ± 8.0 years; 51.3% were female and the primary diagnosis was HgbSS disease (61.5% of diagnoses). The mean number of visits was 1.5 visits per patient with a range of 1–8 visits, both pre and post order set implementation. Thirty-one patients had ED visits at both time periods.
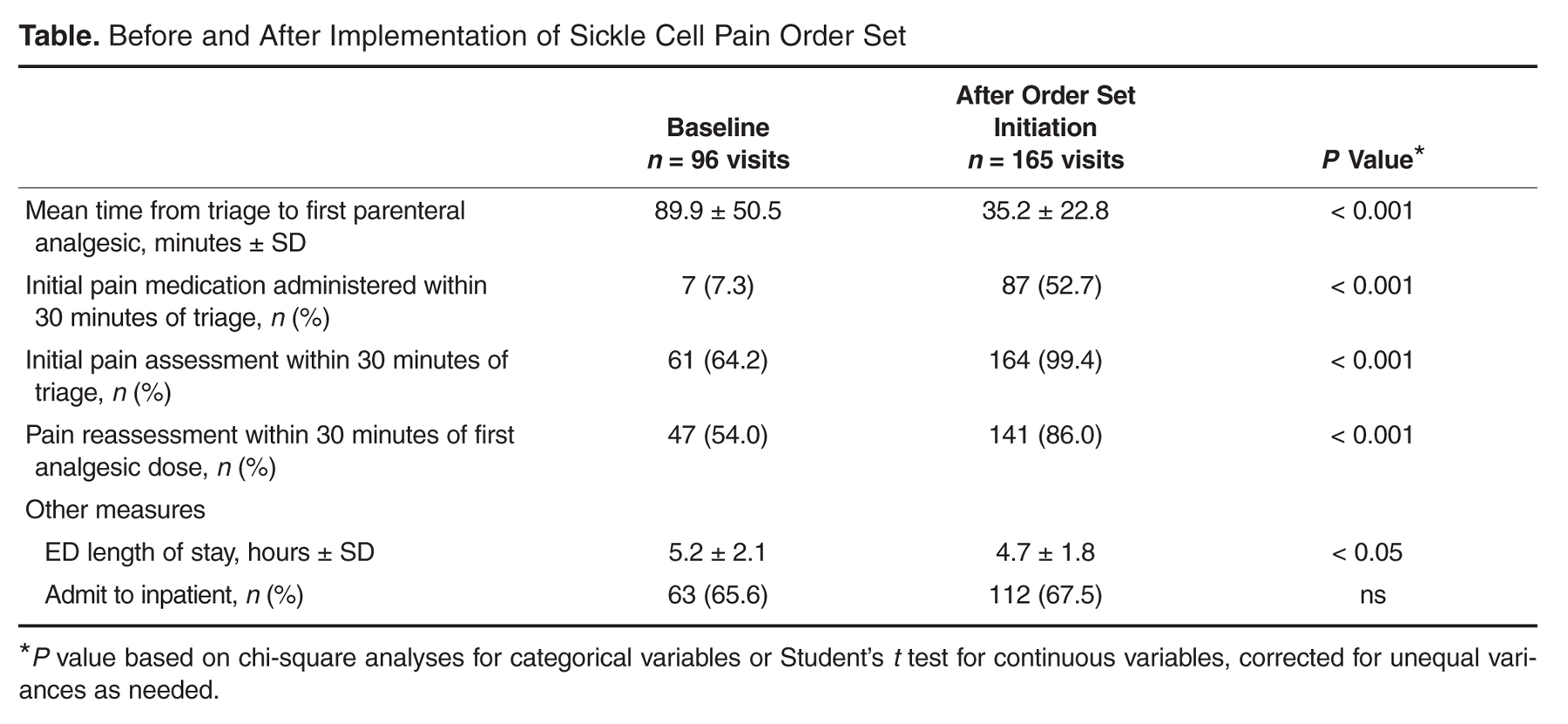
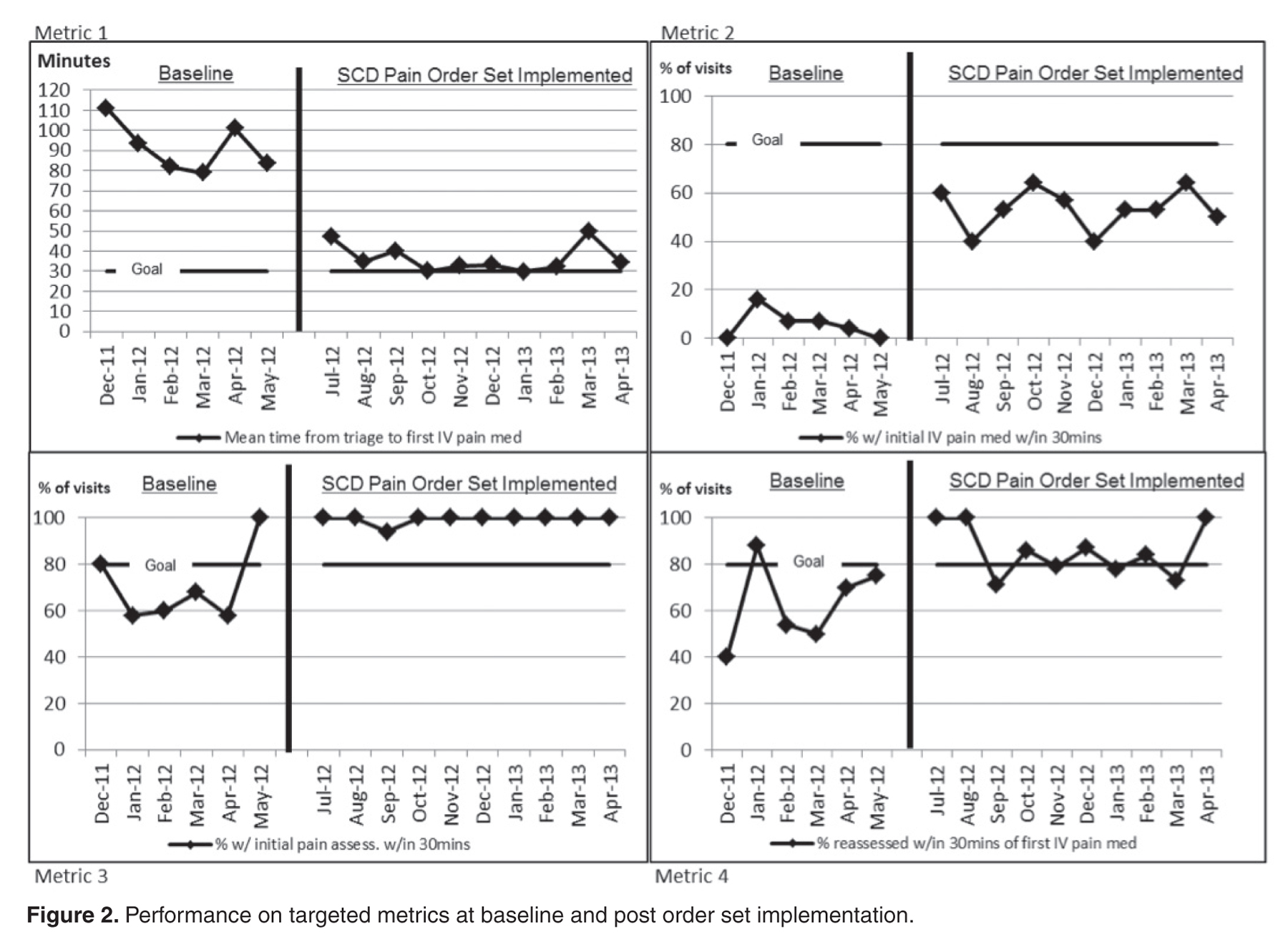
Statistically significant improvements were seen for all targeted metrics ( Table). Time from triage to administration of first analgesic dose decreased from 89.9 ± 50.5 minutes to 35.2 ± 22.8 minutes ( P < 0.001) and showed sustained improvement through the duration of the project (Figure 2). Results of Dunnett’s test for multiple comparisons showed that time from triage to administration of first analgesic dose differed significantly for visits during all months post order set implementation compared with baseline (β = –6.0 ± 0.7, P < 0.01). For metric 2, percentage of visits with initial pain medication administered within 30 minutes of triage, we found that all months post order set implementation were significantly different from baseline ( P < 0.001, Figure 2 ). At 53% of patient visits initial pain medication was received within 30 minutes of triage compared with only 7% of patient visits at baseline ( P < 0.001, Table).
For metric 3, percentage of visits with initial pain assessment within 30 minutes of triage, a model was not developed to assess the changes over time given that 100% of visits post order set implementation had the initial pain assessment within 30 minutes of triage, with the exception of one visit in September 2012 (Figure 2). Only 64% of patient visits at baseline were assessed within 30 minutes of triage ( P < 0.001, Table). For metric 4, 3 of the months post order set implementation had 100% of visits re-assessed within 30 minutes of the first IV pain medication (Figure 2). For the remaining months, there was a significant increase from baseline to post order set implementation in percentage of visits re-assessed within 30 minutes of the first IV pain medication (mean of 54% of visits at baseline overall compared with mean of 86% of visits overall post order set implementation, P